Bell’s Palsy
a paralysis of cranial nerve VII (the facial nerve) resulting in inability to control facial muscles on the affected side.
Several conditions can cause a facial paralysis, such as brain tumor, stroke, and Lyme disease.

Ankle Clonus
a neurological finding observed as a spasmodic reflex of involuntary muscular contractions in the ankle due to a compression or injury of the spinal cord.

Muscular dystrophy
a group of hereditary muscle diseases that weaken the muscles that move the human body. Muscular dystrophies are characterized by progressive skeletal muscle weakness, defects in muscle proteins, and the death of muscle cells and tissue
Etiology
- X linked recessive genetic disorder
Manifestations:
- progressive skeletal muscle degeneration
- pseudohypertrophy (muscle tissue replace with adipose and connective tissue)
- muscle atrophy
- muscle necrosis
Posture and Movement:

Several forms of muscular dystrophy characterized by:
- rate of progression
- mode of inheritance
- muscle groups involved
- onset ageeg. Duchenne’s Muscular dystrophy
Pathophysiology
- contractile muscular filament dysfunction
- mutation in dystrophin, a cell membrane protein
- dystrophin coordinates muscle filaments
- dystrophin does not act to attach filaments together
- loose, uncoordinated movement results in intramuscular trauma and inflammation
- poor muscular repair and regeneration processes
- muscle necrosis occurs
- muscle replaced with adipose and connective tissue
Manifestations
- presents around 2 years of age
- muscle weakness
- muscle wasting – atrophy and metaplasia
- disability
- cardiac muscle affected
- smooth muscle not affected
- dyspnea as chest muscles are affected
- cardiac or respiratory complications may lead to death
Dx:
- Hx
- voluntary movement analysis
- muscle biopsy
- increased serum CK – skeletal marker subset analyzed
Tx:
- no cure
- comfort measures
- increase fx
- supportive and symptom management
Myotonic dystrophy (Myotonia atrophica or Steinert’s disease )
chronic, slowly progressive neuromuscular disease
Etiology:
- genetic autosomal dominant disorder
- severe form of muscular dystrophy
- symptom severity increases and onset age decrease with increased mutuated copies (the number of repeats) of the gene carried by the individual

Manifestations:
- weakness and muscular wasting that affects the face and feet and hands and neck
- dysphasia
- typically difficulty with the hands progresses inferiorly affecting arms and shoulders and legs and hips.
.jpg)
Onset and progression:
- highly variable multisystemic disorder.
- slow progression
Management and treatment
the disease is progressive
management and treatment of symptoms and complications as they arise.
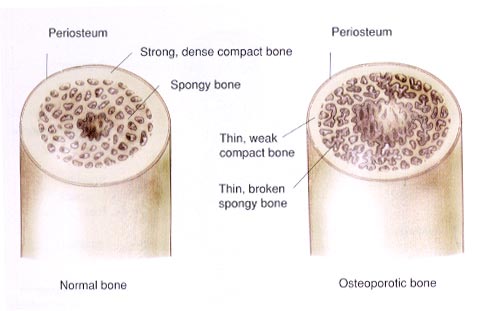
Osteoporosis

- A condition that is characterized by a decrease in bone mass and density, causing bones to become fragile, increasing insufficiency fracture risk
Etiology:
- aging
- genetics
- endocrine disorders – parathyroid hormone changes,
- hormonal profile changes – menopause
Most Crucial Risk Factors
- low peak bone mass
- increased bone loss post menopause – estrogen loss
- aging: post 30yrs – bone mass loss
Pathophysiology:
- the cycle of osseous remodeling changes with age (decreased osteoblast activity)
- 20yrs of age – all epiphysial plates fused
- resorption begins to overtake osteoblast activity post 30yrs
Manifestations
- musculoskeletal pain of bones and muscles d/t microfractures
- vertebral changes – compression #’s, kyphosis
- mandible deterioration – dental loosening and loss with increased bone resorption periodontally
Dx:
- bone density scan of
- hip
- wrist
- spine
- photon detection as radiation passed though bones
Tx:
- vitamin and mineral supplements
- excercise
- fracture prevention
- pharmacologic interventions – decrease rate of bone resorption
Arthritis
inflammation of joints due to infectious, metabolic, or autoimmune causes resulting in pain, stiffness and limitation of motion of the affected joint.

Pathophysiology
- affects synovial joints
- characterized by inflammation and degeneration of the joint
- antigen complexes adhere to joint surfaces
- phagocytosis of the immune complexes result in tisue estruction
- phagocytosis produces leukotrienes and prostaglandins which determine the level of inflammation
- prostaglandins produce collagenase degrading collagen in the joints

Menchanical stress
- repetitive impact loading results in cartilage destruction
- walking transimts 3-4 times the body weight to the knee
- repeated mechanical stress decreases elastiticity of ligaments and articular cartilage
- the joints shock absorbancy declines
- thining of subchrondral bone results
- joint stability overall decreases
- osteophytes form
- synovial capsule and membrane thicken
- joint cartilage atrophies
Joint lubrication:
- declines as mechanisms that normally operate under high weight loads to produce joint lubricating film decline.
Immobilization of a joint
- may result in joint degeneration
- cartilage degeneration may result from loss of lubrication flow within the joint capsule with lack of mechanical movement.
Clinical Manifestation
- pain
- joint swelling
- limited movement
- stiffness
- weakness
- fatigue
Assessment
- Hx of symptom evolution and onset
- previous tx and effectiveness
- fx assessment
- gait
- posture
- musculoskeletal size and structure
- gross deformities and abnormalities noted
- symmetry, size and contour of other connective tissues
- reported abilities vs observable functioning
Dx:
- ESR – erythrocyte sedimentation rate – indicative of degree of inflammation
- arthrocentesis – relieve pressure and analysis for infection (rule out infectious arthritis or tx gout)
- X-ray – joint changes
- Arthrography – detect connective tissue disorder
- Bone and Joint scan – indicative of bone density in affected region and joint degeneration
- Tissue biopsies – myositis, vascular changes
- blood test – auto-Abs
Geri:
- individual may expect limitations with aging as normal
- OA increases in prevalence with aging
- pharmacologic intervention SE intensifies in the elderly
Management
- involves multidisciplinary team
Pharmacologic intervention
- symptom management and anti-inflammatories
- Salicylates
- NSAIDs
- antirheumatics
- pain management
- sleep aids – promote adequate and normal sleep pattern
Additional management
- heat and cold packs
- protective splinting
- supportive devices
- maintain low impact regular ROM excercise

